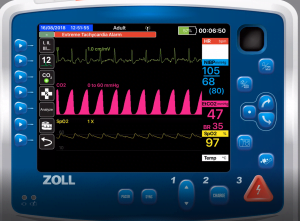
The image shows a significantly widened alpha angle, also referred to as “shark fin” capnography waves. (Photo courtesy iSimulate.com)
On the go? Listen to the article in the player below!
CPAP (Continuous Positive Airway Pressure) is a valuable tool for a wide variety of patients with acute shortness of breath. There are very few reasons why any acutely dyspneic patient should not have at least a trial of CPAP. In some situations, such as acute pulmonary edema, the beneficial effects of CPAP become apparent within seconds to minutes. In others (probably comprising the majority of BLS and ALS CPAP applications), it can be challenging to determine whether CPAP is helping, not making a difference or potentially harming your patient. A very valuable, but often underused tool for evaluating the effectiveness of CPAP is capnography. This column will explain how you can use end tidal CO2 measurements to titrate and evaluate the effectiveness of CPAP.
Capnography is the non-invasive measurement of exhaled carbon dioxide (CO2) displayed as a CO2 waveform concentration over time. During the 1980s, capnography became a standard for anesthesia care in the U.S.,1 virtually eliminating misplaced invasive and supraglottic airways. Capnography reflects ventilation, perfusion, and metabolism; alternatively, pulse oximetry mirrors oxygenation status. In steady cardiac output and metabolic states, CO2 production remains relatively constant, hence measuring exhaled CO2 directly reflects ventilation. Capnography is available for both spontaneously breathing patients and patients who are receiving positive pressure ventilation.
For patients who are breathing spontaneously, exhaled CO2 can be measured using a nasal cannula type device where one of the cannula prongs (and sometimes an additional collector positioned over the mouth, referred to as an “oral pillow,”) samples respiratory gases. For patients receiving positive pressure ventilation, CO2 is measured using an adapter placed at the connection between the ventilation device or circuit and the advanced airway or mask being used on the patient. In BVM ventilation with a continuous mask seal maintained during exhalations, accurate CO2 values and waveforms will be displayed when using an adapter connected between the bag and mask.
Unlike BVM ventilation, the high gas flows generated during non-invasive ventilation (NIV) such as CPAP or BiPAP significantly washout CO2. To obtain accurate CO2 measurements and waveforms while using NIV, sampling must be done using the nasal oral site with a cannula type device that incorporates an oral pillow (mentioned previously).2-4 The cannula type device should be placed prior to applying the NIV mask. The air leak resulting from the extrusion of the cannula under the mask is minimal and readily overcome by the high gas flows used.
Once an accurate CO2 measurement is obtained, the numerical value (EtCO2) and waveform can be used to titrate pressures and to assess the effectiveness of other treatments such as bronchodilators.5 Initially and prior to applying CPAP, you will often see higher than normal EtCO2 values (normal 35 – 45 mmHg). In a patient without COPD, an EtCO2 greater than 70 suggests respiratory failure and, while a trial of CPAP is wise to consider, providers should have a very low threshold for assisting ventilations. Normal or low EtCO2 values are often present early in acute respiratory distress, but may also be seen in patients with low cardiac output, extreme acidosis and hyperventilation. These complex clinical differentiations are beyond the scope of this article.
How quickly you see changes in EtCO2 depend on the reason for use. In acute pulmonary edema, you can expect to see EtCO2 values decline rapidly, often over the course of 3-5 minutes. Acute respiratory distress from a pneumonia, exacerbations of COPD or asthma may take much longer to change significantly, often requiring 10 – 15 minutes. This should not stop you from titrating pressures based on patient comfort and the general direction, or trend, the EtCO2 is moving.
Most EMS protocols suggest initial CPAP pressures of eight to 10 CWP for adults. Once in place, pressures can be increased by two-three CWP increments (depending on the device in use) every two-to-three-minutes for comfort and until EtCO2 levels stop increasing or begin to decline. The practical ceiling for CPAP pressures in adults is 20 CWP. Most devices won’t allow higher pressures; patients typically cannot tolerate them and gastric distention from entrainment of air becomes a significant concern above 20 CWP.
The target EtCO2 is the normal range of 35 – 45 mmHg. Just as you should escalate pressures to stop the EtCO2 from climbing, it is equally appropriate to wean pressures when CO2 falls back into normal or below normal range.
Likewise, the capnography waveform should guide your treatment. The image at the top shows a significantly widened alpha angle, also referred to as “shark fin” capnography waves. While CPAP may be helpful, this patient very likely would benefit from a bronchodilator. Once administered, changes in the capnography waveforms will help to determine the effectiveness of treatment and the need for additional medications.
Treating an acutely dyspneic patient is an art and a science. It takes finesse, good patient assessment and communications skills, and the ability to use the tools at your disposal to help your patient. Capnography is one such tool that provides an objective reflection of your patient’s ventilatory status and can help you titrate CPAP for maximal effect.
References
- American Society of Anesthesiologists: Standards for basic anesthetic monitoring. 2015; [on-line]. Available at asahq.org/standards-and-guidelines/standards-for-basic-anesthetic-monitoring.
- Nuccio PF, Hochstetler G, and Jackson M. End-tidal CO2 with noninvasive ventilation. Journal of the International Anesthesia Research Society 2007;105:S111.
- Nuccio PF, Hochstetler G, and Jackson M. End-tidal CO2 measurements with noninvasive ventilation. Innovations and Applications of Monitoring Oxygenation & Ventilation (IAMOV) International Symposium at Duke University 2007.
- Defilippis V, D’Antini D, Cinnella G, Dambrosio M, Schiraldi F, Procacci V. End-tidal arterial CO2 partial pressure gradient in patients with severe hypercapnia undergoing noninvasive ventilation. Open Access Emergency Medicine. 2013; 5:1-7.
- Orr J, Jaffe MB, Seiver A. Capnography in non-invasive positive pressure ventilation in Capnography, 2e. Cambridge, England: Cambridge University Press. 2011. 135-144.

Mike McEvoy, PhD, NRP, RN, CCRN, is the EMS coordinator for Saratoga County, New York, and the professional development coordinator for Clifton Park and Halfmoon Ambulance. He is a nurse clinician in the adult and pediatric cardiac surgery intensive care units at Albany Medical Center, where he also teaches critical care medicine. McEvoy is the chief medical officer and firefighter/paramedic for West Crescent Fire Department in Clifton, New York. He is also the chair of the EMS Section board of directors for the International Association of Fire Chiefs and a member of the New York State Governor’s EMS Advisory Council. He is a lead author of the textbook Critical Care Transport, the “Informed” Pocket References (Jones & Bartlett), and the American Academy of Pediatrics textbook Pediatric Education for Prehospital Professionals (PEPP).