All images created by the author.
The weather is finally starting to break, and spring is almost here. It’s that awesome time of year when you get to wear shorts again. You and your partner hop in the rig and head out for dinner, hoping to successfully accomplish that mission as you pull up and park, excited for your spicy beef Pad Kra Pao.
You fall into the excitement as you hear your partner yapping to your left about their inability to comprehend how you can handle the heat of food that spicy, you casually look over, roll your eyes, and remind them that you bask in the joy of sweating and feeling that flushed rush of the capsaicin kicking in and your blood vessels firing up. As you finish your sentence with your silent punctuation, you get a sinking feeling as you hear your CAD chirp.
You’re being dispatched about three miles away for an 82-year-young male who is having breathing problems. The joy of the spice will have to wait; you make en route and head on over to the local skilled nursing facility.
The ride over is only a couple of minutes. You pull up under the ambulance entrance, hop out, grab your bag of tricks and box of life, and head in. You’re pseudo-greeted by a staff member who is down the hallway and yells room 104 to you, but can’t possibly be bothered to come give you a report or any information for that matter.
Around the corner, in room number 104, you find George sitting on the edge of his bed in what feels like an African jungle-temperature room, with the TV on the loudest volume it can produce. Your partner saunters over to the TV and turns it down as you make your way to George, shake his hand, and introduce yourself.
You find he fixes and follows when you walk in the door, shakes your hand with good grip and tone, and also verbally introduces himself, but is broken in between words, of which he can only get one to two out at a time. You reassure him that you’ve got him and that you’re gonna take great care of him with your partner.
You let him know your partner is going to get some vital signs while you listen to Long sounds. You hear the following lung sounds and obtain the following vital signs from your partner, who’s pointing to the box of life.

What are your initial thoughts and concerns?
You let your partner know that you heard wheezing and gesture outward on expiration. And you ask George if he has any lung problems. He shakes his head yes and says, “A… couple….” you take a glance back at the monitor and ask your partner for a 15-lead and take a quick step over to the door to poke your head out looking for any of the clinical historians/staff/helpers/or really any form of life in the hallway that might be of any assistance to giving you some backstory on George.
You see one way down the hallway, but it appears to be about a quarter mile, and it eerily feels like the movie “The Shining.” You holler down for a face sheet and are told one second, so you hop back into the room, take a peek at the 15-lead, and ask your partner to get a nebulizer ready.
Your partner also took the liberty, as great partners do, of gathering some additional data on George and presenting the following to you. You hear your partner ask George whether he knows his normal pulse ox level. Out of the corner of your eye, you see George shake his head yes and state 92%.
You prompt George to focus on breathing, then ask him some questions and have him give you a thumbs-up or thumbs-down for each one. He gives you a thumbs up. You ask George whether this trouble breathing came on quickly (thumbs up) or has been going on for a little while (thumbs down).
He gestures the number two to you; you expand, asking if he means, by number two, it’s been a while, and he nods yes. You ask for a couple of hours, a couple of days, a couple of weeks, and again, he gives you the number two. And you confirm a couple of days, and he shakes his head yes.
Your partner starts the nebulizer, and you ask if they put Atrovent in it. They say yes, you ask if they can dump that and just do a single albuterol to see if that turns him around. They agree and go back to the bar to mix up the nebulizer cocktail. At about the same time, the staff member rolls in with the face sheet and passes it off to you like a football from Troy Aikman to Emmitt Smith.
As you’re reading through the novel about George, you let him know that he’s going to get some medicine to breathe in, and that you’re gonna take a peek at his batting average stats and his paperwork, and he subtly chuckles, while your partner is putting the nebulizer on his face.
You find his history sheet, the usual cocktail of blood pressure medicines, cholesterol medicines, a multivitamin, gout medication, prostate medication, and even more that don’t pertain anymore, but still reside in the record from times of infection, electrolyte balance issues, rashes, etc. He also has steroids and a multidose inhaler.
So, what do you think is going on with George?
Your partner recycles the pressure and points over to the box of life while you finish reading the novel. As you start to glance over, you also ask George if he feels better, and you see him nod and say, “Yes, I do,” over the sound of that nebulized mask.

Is he better?
You again make your way to the hallway, looking for any sign of life, and again find none. You ask George if it’s OK if you take him up to the hospital because the medication you gave him to make him feel better is not long-acting, and you’d like him to get his lungs and labs assessed.
He says without hesitation, “Yes, please, anything to get me out of this place,” in clear, crisp, complete sentences. You look right back at him, acknowledging his ultra willfulness to get out and escape. Your partner wheels the cot in, you help George get him loaded up, and head on over to University.
Talking to George en route and finding out about how just badass of a dude he is from his childhood on a farm to his service in World War II, starting at the age of 16 when he lied on his recruiting application.
You jokingly let him know that if he’s interested, your agency is hiring and you’d love to have a person with that type of motivation and work ethic, and he looks over from the corner of his mask, smiling, stating, “Oh, I would if I could!”
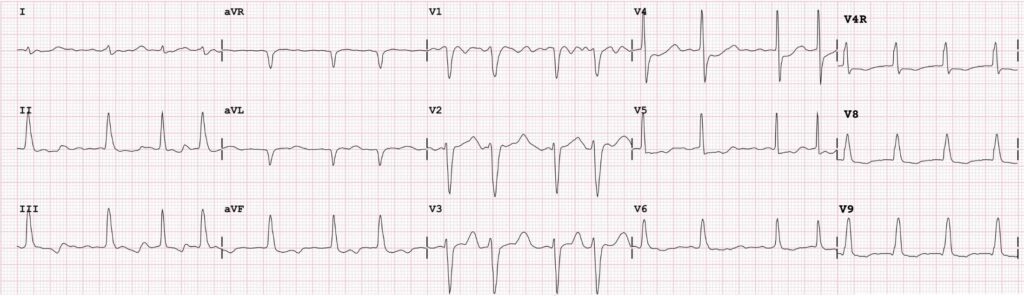
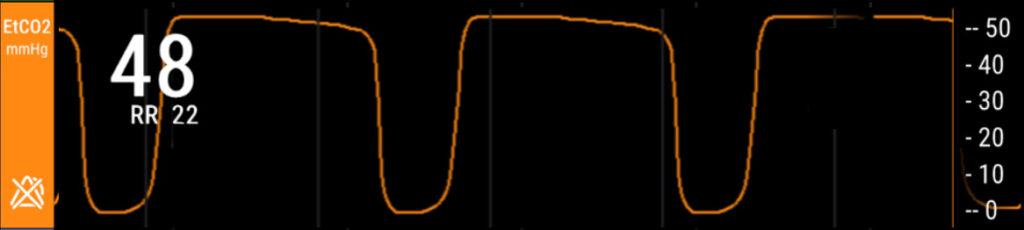
So, what is going on with George, and why the wheezing? And why the weird wave on his end tidal after you got his breathing better?
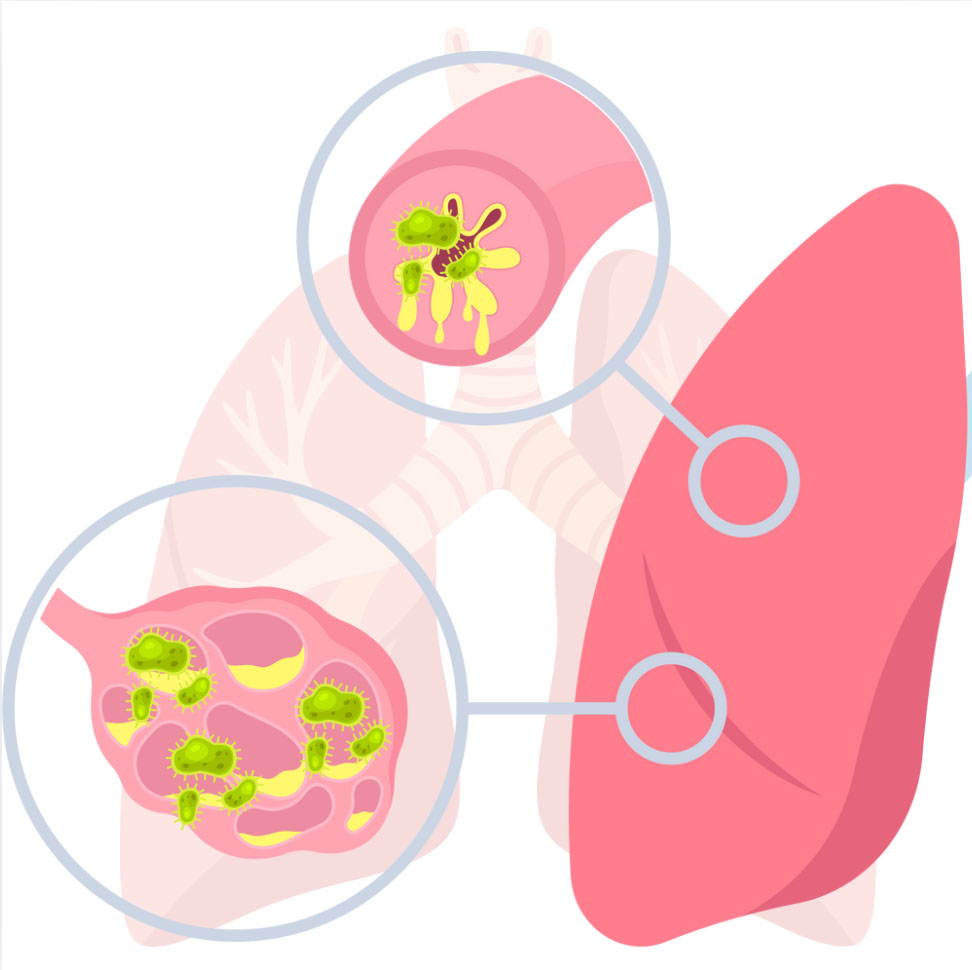
Well, George is an example of a patient with localized pneumonia. Hence, the right-sided lower lobe wheezing, which was less prominent on the left, and what you likely heard was resonance from the right to the left, almost like a carryover echo. With pneumonia, because there is localized inflammation and irritation at the site of the infection/petri dish, you can get bronchospasm, inflammation, swelling, etc., so you get wheezing, usually around the area where the problem is occurring.

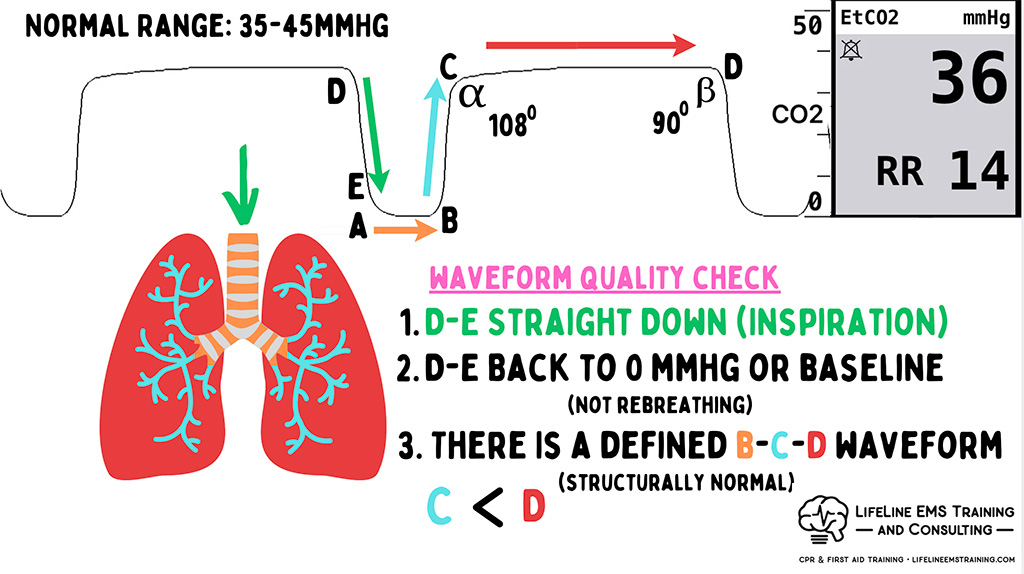
But what you don’t get is a global impact on your entire waveform. Because the end-tidal wave is the sum of all airways, if the person were experiencing a global asthma attack or an anaphylactic reaction, we would see the impact on the C phase of the wave.
In George’s case, he has a localized infection to one or potentially two lobes on one side of his body, so we didn’t see that change on the end-tidal.
In otherwise healthy lungs that experience pneumonia in a large area, you may see slight rounding of the sea face, because in otherwise healthy lungs, it is enough to have a net impact on that form.
But in George’s case, he has another underlying condition that alters the wave, and instead of rounding the C phase, it enhances it, making it more prominent than in individuals without this condition.
What you saw in his second vital sign assessment after you’ve assisted opening up his airways, especially those in the areas that are inflamed and infected, is that he has a baseline reverse (beta) wave, and so his C phase is greater than his D phase.
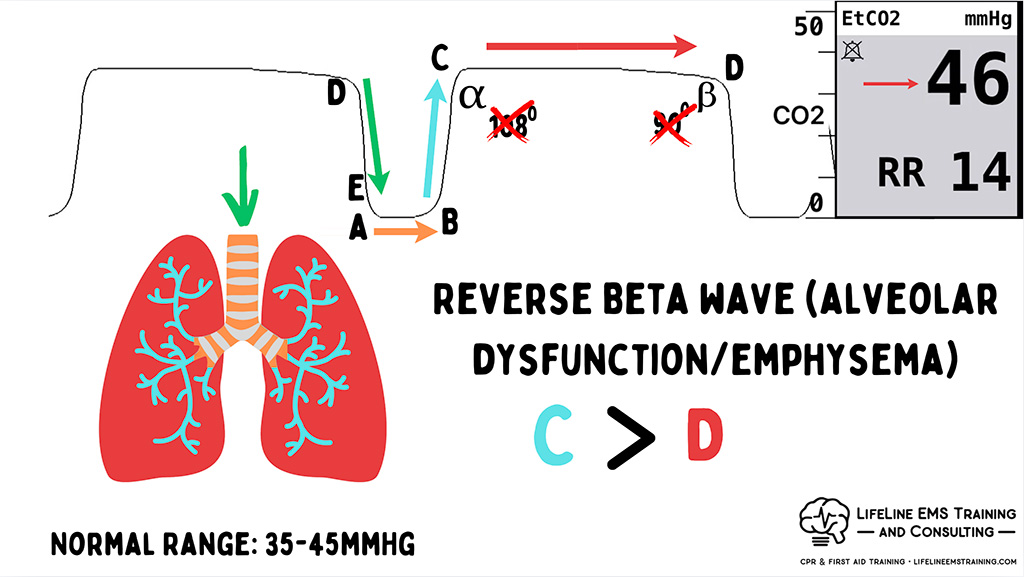
This is a manifestation of a structural issue in his lungs. And that structural issue has occurred over time from the smoking he’s been doing since he was 16, and the issue is that George has emphysema, pretty prominent emphysema, actually. So what you see is that C (bronchioles) holds more carbon dioxide than D (alveoli).
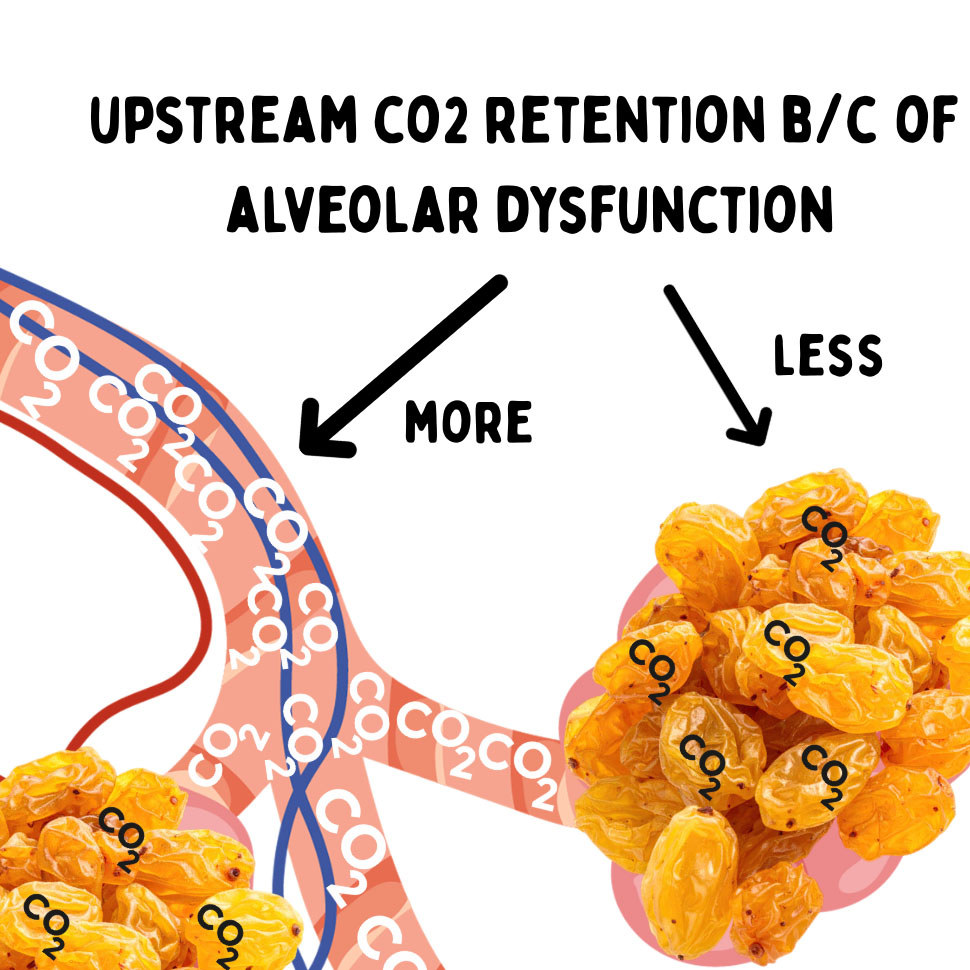
So, we can use this waveform to help us recognize that he has alveolar dysfunction, and that those alveoli are not as sack-like or bag-like as they should be. They are not holding the majority of that CO2 at the point of gas exchange. They’re like sad raisins, and that CO2 is being held upstream in the bronchioles.
This waveform is not uncommon in patients who have severe emphysema or individuals who have had a cold smoke inhalation and have damaged their alveoli.
Specifically, the surfactant and elastin in the alveolar wall give it balloon-like properties. In George’s instance, his normal is probably a slightly elevated end tidal every day, all day, with a C greater than D.
And in his case today, he has a localized infection requiring more respiratory workload to get gas past points of infectious resistance (think infectious pinching of the airway), and that tipped him over the edge.
What we found was that a little bit of nebulizer and some TLC helped him through this. If he was not oxygenating adequately for us, and remember with COPD’s adequately is at or around their baseline, and he wasn’t turning around on us. We would want to support the alveolar structure and function by helping it maintain volume, and we would consider options like CPAP in this case, but George did well with 8 L per minute via nebulizer, with the medication assisting his bronchial opening, reducing resistance, and easing his work of breathing.
We also have some extra confirmation that helps our backstory with George: his infection, the slightly elevated blood sugar (with no history of diabetes), the slightly elevated temp from a gentleman who didn’t just get off the treadmill or run a marathon, and the lung sounds are localized.
We also know he doesn’t have a markedly high diastolic pressure and non-global lung sounds, which are more consistent with an event that came on all of a sudden vs ours, which has been cooking over time. Those criteria will lead us to worry about cardiac wheezing versus pneumonia wheezing.

Chris Kroboth has been a career paramedic/firefighter for over 17 years and in EMS for over 23. He has been in prehospital and in-hospital education for the past 18 years. His last assignment before returning to operations was as the EMS training captain in charge of continuing education programs and certification. He is also affiliate faculty with the Virginia Commonwealth University Paramedic Program. He is the U.S. clinical education manager for iSimulate and also facilitates national conference clinical challenges to include EMS World, ENA and NTI.