
A First in Nepal: A Patient Intubated Inside a Fixed-Wing Aircraft
The mission was to bring a 47-year-old male patient from Biratnagar to the Hospital for Advanced Medicine and Surgery in Kathmandu, Nepal.
The mission was to bring a 47-year-old male patient from Biratnagar to the Hospital for Advanced Medicine and Surgery in Kathmandu, Nepal.
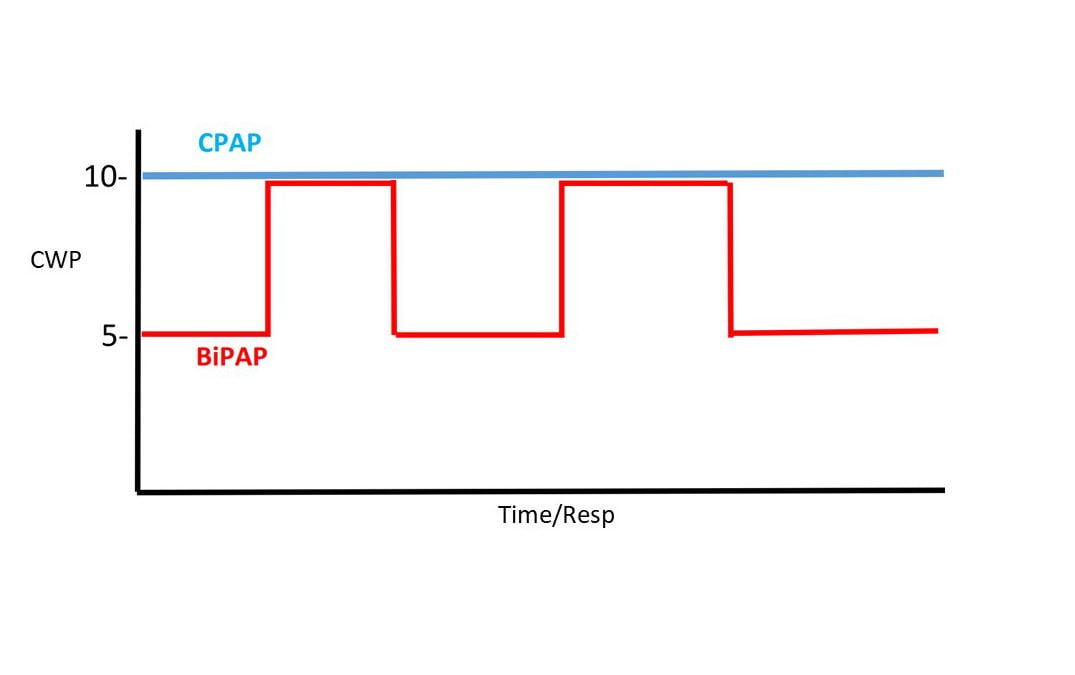
This article reviews the essentials of BiPAP, how it differs from CPAP, and summarizes potential advantages and disadvantages.

Patients suffering from infection with SARS-CoV-2 are particularly prone to the development of serious respiratory complications.

The authors comment on the prehospital airway debate at the 2020 NAEMSP Annual Meeting.
Many factors go into the equation for deciding between CPAP and BiPAP for a patient.

Measuring EtCO2 is the most accurate monitoring tool that paramedics can use in real time to assess the overall status of the patient in the field.
Recent Comments