
Images provided by the author.
It’s another Friday night with your favorite partner of the century and that proverbial time of year when it’s toasty warm during the day and freezing at night.
You grab a cup of your favorite pour-over coffee with two extra shots to help you through the night. You begin to catch up with your partner on their life events and bounce back and forth about your first-world problems, having not seen each other in over a week.
Just as your jealousy starts to climb from hearing about their tropical vacation and the turquoise blue water they snorkeled in all last week, the CAD chirps. You’re being dispatched to a 32-year-old unconscious female who has agonal breathing.
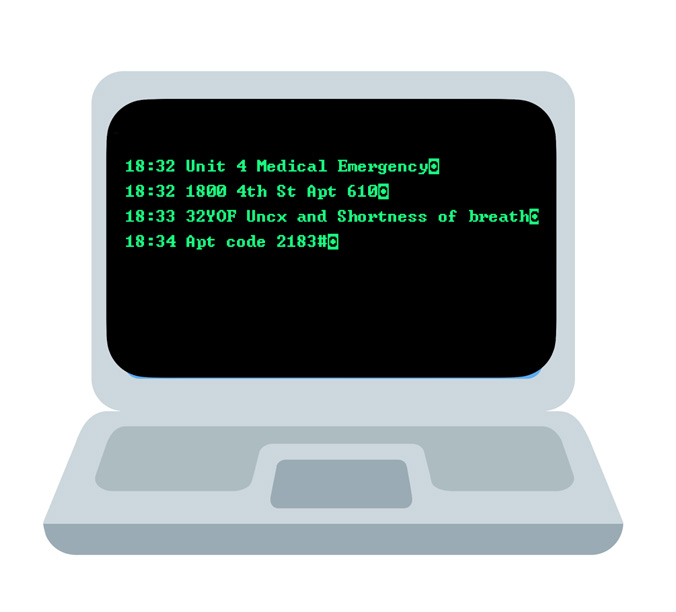
You mark en route and start that way, giving your turn-by-turn directions like the Garmin partner you are. You arrive on scene at the mid-rise apartment complex, gather the access code in the CAD notes, grab your gear, and make your way to apartment 610.
After a short elevator ride, you’re greeted by a frantic male who continues to gesture and voice. “She’s in here, she’s in here.” You are guided through a labyrinth of minimalist modern apartment hallways and rooms and around the corner to what appears to be the bedroom.
You find a young female in bed on her left side, mumbling but breathing. Your partner makes their way to the patient, and you start getting to know the male who met you at the door by asking about his relation to the patient and what is happening.
He says she is 30 weeks pregnant with a boy named Lucas. (You asked the name to help de-escalate and deflect some of the stress running through the spouse).
He says his name is Tom, and that is his wife. You ask if this is her first child, how many times she has been pregnant, and if she has seen an obstetrician for prenatal care and monitoring.
He said this is their first pregnancy, and Lucas will be their first child. They’ve had no other complications, and she’s been going to the obstetrician as prescribed. You hear in the background your partner talking to the patient and her replying with just mumbling.
You turn back to Tom and ask him how long this has been going on, when was the last time he saw her normal, and if there are any other complications he can think of.
He said she had the norovirus the last two or three days and had been vomiting with diarrhea, and he walked in this morning after going to the gym and found her this way. He left her this morning when he went to the gym, and she was still asleep; he said he thought she was sleeping deeply and dreaming because she was breathing heavily.
Your partner turns the monitor toward you.

What are your concerns?
You turn back to Tom and follow up on some of his statements with questions about the norovirus symptoms and what other problems she has been experiencing.
He said, “None, just the stomach bug, and she’s been very weak since that started.” She’s typically very outgoing, and they go for evening walks, but she hasn’t had the energy in the last couple of days. Again, your partner turns to you with some physiological findings.
What are your five differential diagnoses based on the patient’s presentation and vital signs?
You asked Tom if there was any new medication she started, a new vitamin she started, a new diet she started, or any other intake or physical changes that he has noted. He denies all.
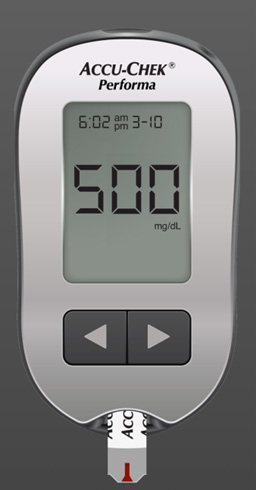
Your partner looks at you and gives the trigger finger gesture, signaling do you want me to start an IV? You nod yes and give them the 5 0 0 with your hand, indicating a 500 ML bolus to start.
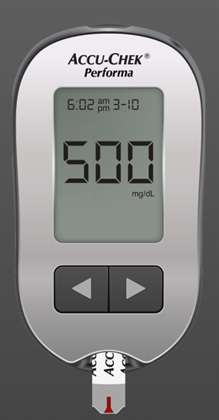
You let Tom know that it looks like her blood sugar is elevated, and you are going to work to get it diluted with some IV fluid. You ask
Tom which hospital they were planning to have Lucas at. He states University because that is where her obstetrician is affiliated.
You let him know you will take her to University and get her checked out. Your partner starts the IV and wraps the bag with a blood pressure cuff to quickly get the fluid going in. You roll Mary onto your stretcher, lift her to the cot, gather your equipment, and start heading down to the unit in the unit.
Your 500 ML bolus has finished, and you have the following vital signs.

You run the vital signs past your partner again, and both agree that another bolus is warranted. You start the second bonus and call in your report to the university, stating that you have a 30-year-old female who is 30 weeks pregnant with what appears to be DKA.
You have your second bolus going, and the patient’s mentation is still mumbling but alert to verbal. You rattle the vital signs and give a six-minute ETA.
So, what do we see here with Mary? We have a young pregnant female with first pregnancy, no prior miscarriages and no current complications. She is not struggling with gestational diabetes. Why would Mary go into DKA, and what vital signs help us lead down that path?
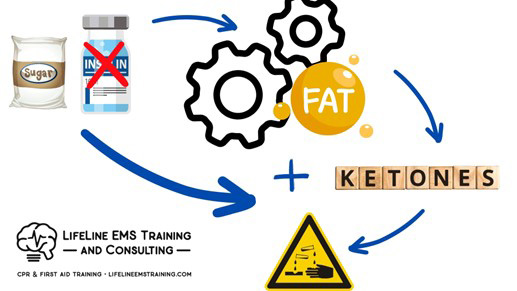
When someone goes into DKA, they do so because they’re not generating enough insulin, and their body starts to break down fat for energy. This breakdown also releases ketones, so we get elevated sugar and ketones. Pregnancy can trigger DKA.
Now that sugar increases in the bloodstream, it creates a hypertonic solution, which the body tries to get rid of through the urinary tract by drawing fluid into the vasculature to dilute the system and excrete it out of the kidneys. The body can only do that for so long before it becomes grossly dehydrated.
It isn’t that uncommon for us to be dispatched to “trouble breathing” or “shortness of breath” when a DKA patient. They are tachypneic from blowing down the CO2 (compensatory) due to metabolic acidosis and ketone buildup.
They are also increasing their respiratory rate to try and help draw blood back into the thorax to the right side of their heart in a dehydrated or low-volume state. Because they start to become bicarbonate depleted from the slow but steady metabolic acidosis, their hydrogen ion levels go up, and CO2 production goes down from the lack of the below reaction:
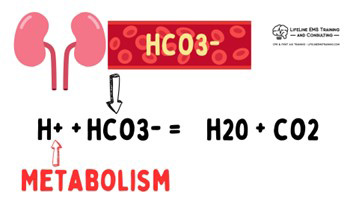
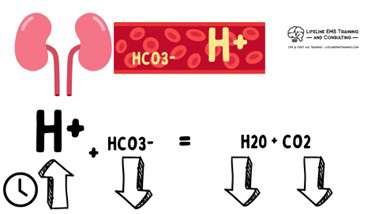
Prolonged metabolic acidosis or reduced bicarbonate production from renal impairment. (Kidneys are super underappreciated.)
So, when differentiating sepsis from DKA. It can be very challenging as their physiological patterns have a lot of similarities, from metabolic acidosis, tachypnea, and tachycardia to elevated blood sugar. But unlike in sepsis, where the elevated sugar is from a cortisol release, in DKA, sugars are very high along with ketone release.
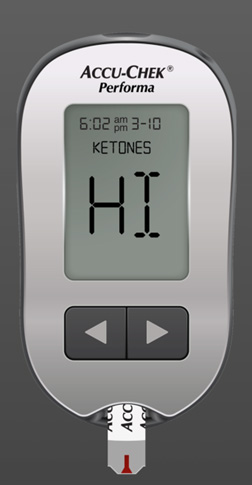
Depending on which monitor you use, you may get a “HI” statement, meaning your glucometer maxes out at a certain threshold and just notes “HI” or a number. We highly encourage you to pull out the pamphlet with your glucometer and read what yours tops out at. Knowing that if it stops giving numerics at 500 and says HI, you cannot discern if it’s 501 or 788. Some glucometers will also test and denote the presence of ketones.
Another thing to look for is skin turgor. Is the skin very dry? Does it stay in place when you pinch it?

You see this commonly in dehydration. In sepsis, patients tend to get puffy or third space from the histamine release and capillary leakage, versus DKA, where they become dehydrated from the shifting of volume from the tissue to the vasculature for the hemodilution.
Like anything in medicine, this is not absolute. In Mary’s case, was it norovirus that then led to DKA, or was it DKA all along, and the vomiting and diarrhea just her body trying to get rid of the elevated sugar?
Chicken or egg in our world, and this case, it doesn’t matter as long as we treat the patient’s physiologic needs.
A good thing to remember is episodes of diarrhea not only dehydrate but also deplete electrolytes!
One last note with DKA is many agencies have used capnography to protocolize treatment based on severity. An example below is the Miami-Dade (FL) Fire Rescue Department, which uses capnography as a definer for treatment and transport decisions based on the patient’s severity and disease progression.
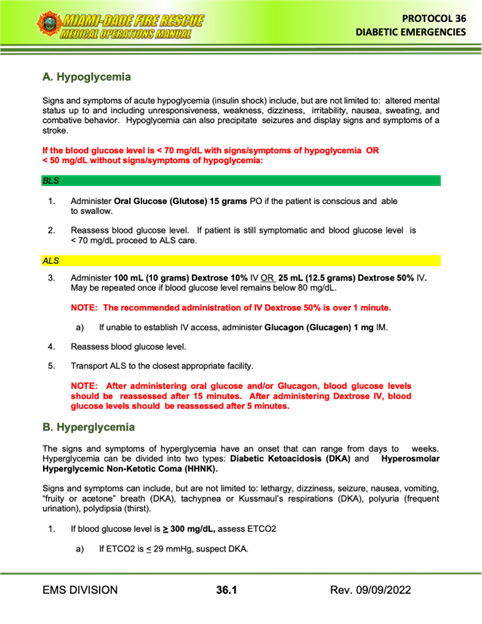
This is another excellent example of how capnography can help you monitor your patient’s criticality and stratify your differentials.

Chris Kroboth has been a career paramedic/firefighter for over 17 years and in EMS for over 23. He has been in prehospital and in-hospital education for the past 18 years. His last assignment before returning to operations was as the EMS training captain in charge of continuing education programs and certification. He is also affiliate faculty with the Virginia Commonwealth University Paramedic Program. He is the U.S. clinical education manager for iSimulate and also facilitates national conference clinical challenges to include EMS World, ENA and NTI.