
All images provided by the author.
How many pillows do you sleep on at night? Are you a one-pillow, two-pillow, full-body, or wedge pillow type of person?

Next question: How many pillows do you put under the patient’s head when you manage their airway?
So, why do we put pillows under our heads when we fall asleep at night? We do that because it helps align our airway, reducing resistance to breathing. Because when we go to bed at night, our parasympathetic system kicks in, reducing our respiratory rate, tidal volume, and metabolism.
By streamlining our airway and reducing resistance, we make our breathing cycle better. If you have obstructive sleep apnea (it’s in the name) or other geometric complications like a large belly, chest, or neck that inhibits your ability to align that airway, as seen in the image below, it can complicate the geometry and, in turn, the flow and ease.
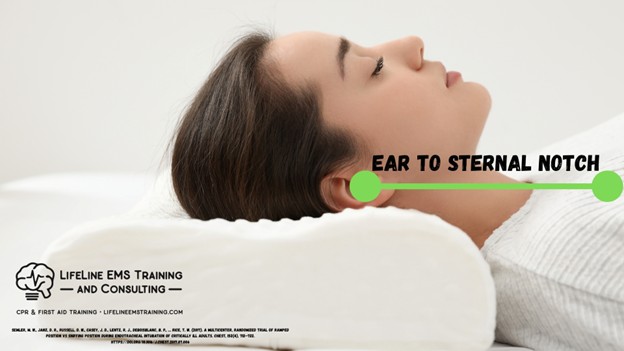
Then you don’t get that easy airflow; you inhibit or block the path, and you get those periods of apnea, and you don’t get the benefit of the rest-and-digest stages of sleep. As you can see in the image below, aligning the ear with the sternal notch is key to optimizing airway geometry and ease of breathing.
Now, close your eyes and reflect on the last one to five patients you’ve managed where you’ve had to support their ventilation. I’m sure you were probably crammed in the bathroom or in the corner of a small room where the person has an aggressive hoarding collection, and you had their head completely flat to the ground, as you smashed the BVM onto their face and tried to squeeze every ounce of air from the bag into their lungs.

Look familiar? Also, remember to pull them out into an area where you can manage them effectively. Don’t play airway TWISTER, trying to pretzel yourself into a corner.
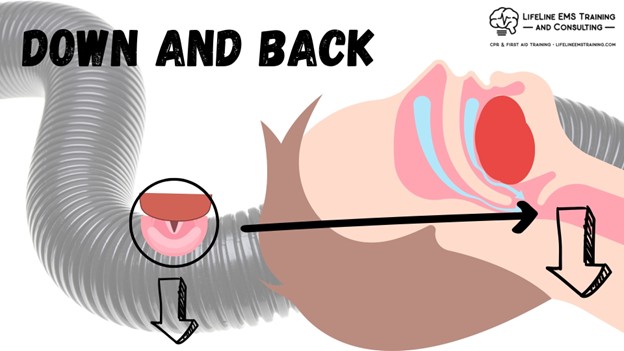
What we find is that by increasing the airflow resistance by actually having the head down versus up, the majority of our air ends up going into the soft, squishy esophagus because that’s now the streamlined path, and what we don’t get is air in and out of the lungs, as seen here.
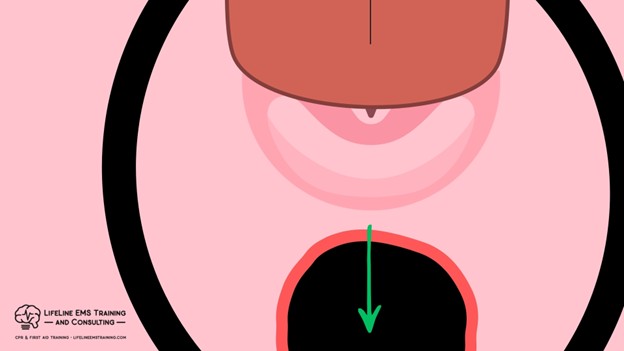
The more air we put into the esophagus, the more volume goes into the stomach; the less diaphragmatic range is available; and we can’t get good tidal volumes into and out of the patient’s lungs.
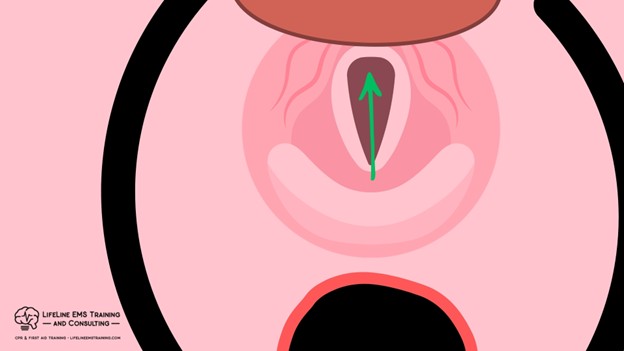
So, some basic geometry for aligning the ear with the sternal notch can optimize low resistance, allowing better ventilation for the patient. This is how any patient you manage without a cervical spine injury should be positioned.
You also get the net benefit of venous dumping from the brain by allowing the head to be slightly above the chest. When in a low perfusion or cardiac arrest state, blood is ejected into the head under left ventricular pressure and/or with compressions.
The venous side is the low-pressure side. The head being above the chest allows for that passive dumping back into the thorax. If the head is down in these low-perfusion or cardiac arrest states, you actually get back up and reduce blood flow to the brain. The lack of venous dumping creates back up and resistance.
I’ll say it one more time. The venous side is the low-pressure side, relying on breathing, motion, and gravity to help it flow, whereas the arterial side is the pressure side. Hence, the venous side has valves, and the arterial side does not.
Now it does not take much to get “most” patients’ ears aligned with their sternal notch. And it does not require a crazy proprietary medical device to do this.
This can be as simple as 2 to 3 hospital blankets rolled up as needed, or one of the 7,333 throw pillows the patient has on their bed or couch, or a stuffed animal adjacent to where the patient is lying, or one of the 10 bags you carry in with you that you’re not using for this patient. Taking that, placing it under the head, and aligning the two points.


I do want you to recognize, however, that this is not taking the patient’s head over the back of the cot (torquing), allowing it to drop down; this is aligning the ear above the sternal notch.
Now, if this is a new concept to you, you are not alone. I distinctly remember, in my initial education, never talking about this, and I also remember being plagued by simulation tools that created scars because they didn’t allow for optimized positioning.
The airway simulator industry is finally starting to wake up to the basics of airway management and preparatory positioning. Below, you’ll see an example of an airway head that allows for multi-access positioning, not torquing the neck back and forth. I know when I was taught, it was to take the patient’s forehead and yank it all the way back, hyperextending the neck. There are a couple of problems with that: number one, it pushes the tongue and closes the glottic opening, and it also puts tension on the lateral muscles of the neck, potentially including jugular venous flow, to name a few.

My challenge to you is: on your next shift, crew day, or your next training day, grab a handful of those awesome 3000-count Egyptian cotton hospital-grade blankets (sarcasm completely inserted) and have your crew members lie flat on the ground and practice their ear with their sternal notch.
You’ll be surprised at the ones you would think would be one or two blankets, and they end up being five, and the ones that you think would be four or five, and end up being 1/2 rolled up. It is very hard to discern neck mobility and range just by looking at a person. Ask them when they’re finally aligned if they can actually breathe better. I guarantee the answer is “oh yes, I can!”
So, please remember that part of airway management is ensuring the patient has their airway pillow and is positioned appropriately. Because you want your squeezes to go in and out of the lungs, not in the stomach and out of the stomach, nobody wants a number one super-sized with fries sprayed all over the crew.


Chris Kroboth has been a career paramedic/firefighter for over 17 years and in EMS for over 23. He has been in prehospital and in-hospital education for the past 18 years. His last assignment before returning to operations was as the EMS training captain in charge of continuing education programs and certification. He is also affiliate faculty with the Virginia Commonwealth University Paramedic Program. He is the U.S. clinical education manager for iSimulate and also facilitates national conference clinical challenges to include EMS World, ENA and NTI.